New Human Physiology | Paulev-Zubieta 2nd Edition
Chapter 5: Special Senses and Disorders
| HOME | PREFACE | TABLE OF CONTENTS | SYMBOLS | SECTION INFO | CONTRIBUTORS | LINKS | CONTACT US |
Highlights
Study_ObjectivesPrinciplesDefinitionsEssentials
PathophysiologyEquationsSelf-AssessmentAnswers
Further Reading
|
|
|
 |
|
|
Astigmatism Cataract Colour blindness Conduction deafness Far-point Glaucoma Hypermetropia Hemianopsia Myopia Near-point Nerve deafness Nystagmus Presbyacusis Presbyopia Receptive field Scotoma Strabismus Transportation sickness Visual accommodation Visual acuity Visual agnosia This paragraph deals with 1. The visual system, and 2. The auditory and vestibular system. This system detects, transmits and interprets photic stimuli. Photic stimuli are electromagnetic waves with wavelengths between 400 and 725 nm. This is visible light or the adequate (effective) stimulus for the eye. The eyes can distinguish brightness and colour. The photoreceptors are rods and cones located in a specialised epithelium called the retina. In each eye the retina contains about 6 million cones and 120 million rods. In the peripheral region of the retina both rods and cones converge on bipolar cells. The bipolar cells converge on ganglion cells giving rise to the one million nerve fibres in each optic nerve. In addition, there are horizontal cells and amacrine cells in the retina. They conduct impulses laterally. Rods and cones Rods are most sensitive in the dark (scotopic vision). More than hundred rods converge on each ganglion cell. There are no rods at all in the fovea. Cones operate best in light (photopic vision). Cones have a high-resolution capacity and hence a high visual acuity, because the light is focused on the fovea, where the cones are concentrated. The high resolution is also due to the small convergence of cones to bipolar cells in the fovea (approximately a 1:1 relationship). Cones are responsible for colour vision. Cones are surrounded by pigment, except where the light enters. The eye contains chamber fluid, which is produced by filtration and secretion in the ciliary processes. The intraocular pressure is normally 1.3-2.6 kPa (10-20 mmHg). Increased resistance to fluid outflow at the iridocorneal junction leads to increased intraocular pressure with loss of optic nerve fibres- or glaucoma. In this condition, the retinal artery is compressed at the optic disc, where it enters the eye. This causes retinal and optic nerve atrophy which eventually results in blindness. A diopter is the unit for the refractive power of a lens. The diopter (D) equals the reciprocal value of the focal length of the lens in metre (m). Visual accommodation is the rise in the refractive power of the lens, obtained as the lens rounds up, because of contraction of the ciliary muscle and relaxation of the zonule fibres. Each object we look at has a special target point (the fixation point), from which light passes un-refracted through the nodal point of the eye and focuses on the fovea, creating the sharpest possible image. The nodal point in the eye is precisely the point through which a light beam passes un-refracted. The far point (F or punctum remotum) for the eye is the fixation point in the un-accomodated eye (Fig. 5-1). The near point (N or punctum proximum) of the eye is the fixation point for a maximally accommodated eye (ie, when the lens is in its most spherical configuration). The refractive power of the lens can vary between 12 and 26 D. The accommodative power of the eye is the rise in refractive power from the un-accomodated to the maximally accommodated condition (see Eq. 5-1). A child of 10 years has 12-14 D, a 20 year old person 10 D, and a 60 year old person only 1 D in accommodative power. The optical distance convention defines all distances measured from a light source to the eye, to be positive. Thus, all distances from the eye to the light source are negative. Hence, the distance from the nodal point of the eye to a point in front of the eye is negative. Convex refractive media bend (convergence) in-falling light behind the media and thus have a positive diopter. Concave lenses have refractive powers with negative Diopters, because the focal point is in front of the lens. Convergence or near vision occurs when the eye focuses on an object closer than 6 m from the eye. Near vision - even with only one eye - triggers accommodation and pupillary constriction. The ciliary muscle and the pupillary sphincter muscle are innervated by the parasympathetic oculomotor nerve, and the two muscles contract simultaneously for near vision. The visual fields of both eyes are perceived as only one continuous visual fields (the Cyclops eye effect). This is fusion or the illusion that we are looking at the world with only one eye. In a healthy eye, the light from an object in the visual scenario is focused sharply on the retina by the cornea and the lens. Both of these refract (bend) light. The cornea has a refractive power of 43 D, and the healthy lens has a refractive power that varies between 12-26 D. Thus the total refractive power is 56-69 D. The lens allows the eye to accommodate, so that both near and distant objects can be focused on the retina and thus clearly seen. When we look at distant objects with normal eyes and relaxed ciliary muscles, the object foveates automatically. However, when we look at nearby objects, the light is initially focused behind the retina. The lens then rounds up, by contraction of the ciliary muscles and relaxation of the zonule fibres (i.e., accommodation), to focus the image on the fovea. The normotropic eye has the ideal refractive power. Parallel light from the far point (F in the upper part of Fig. 5-1) foveates on the retina in the un-accomodated eye. Light from the near point (N in Fig. 5-1) in the totally accommodated eye also foveates.
Fig. 5-1: Hypothetical light rays for emmetropic, myopic, facultative and absolute hypermetropic eyes. The coloured space in front of each eye is the fraction of the three dimensional space, which can be focused on the retina for a given visual axis (Fig. 5-1). Conjugate movements are movements of both eyes in the same direction and magnitude, so that the relation between the visual axes is maintained. When focusing on far away objects, the parallel axes are maintained during conjugate movements. Likewise, conjugate eye movements maintain the convergence angles of the eye required for focusing on nearby objects. Saccadian or jumping movements are rapid eye movements. Saccadian eye movement is an instantaneous reposition of the eye that occurs when reading or when focusing on a flash of light in the peripheral visual field. The velocity of the movement is up to 500o per s. The latency period is 250 ms, and the contraction time is 50 ms. The compensatory eye movement involving the vestibular system, occurs when the head rotates. This is also an example of Saccadian eye movement. In contrast, pursuit movements are smooth eye movements that allow the eye to track a moving object. They have a velocity of up to 30o per s. These two movements work together in optokinetic nystagmus. This is a shift between smooth pursuit movements and correcting jumps. The direction of nystagmus is by convention indicated by the rapid correcting phase. Even during foveation of an object the eyes are not totally still. The eyes are continuously performing miniature eye movements, which occur at a rate of 3 microsaccades per s, with mean amplitude of 0.1o. The number of photoreceptors in a human eye is estimated to be 110-130 million rods and 5-7 million cones. Each photoreceptor cell includes an outer and an inner segment, which are united by a thin cilium. The outer segments are directed towards the pigment epithelium of the peripheral retina, and contain stacks of disks that are rich in photo-pigment molecules. The inner segments contain the cell nucleus and numerous mitochondria. The rods are predominant outside the fovea, and they contain much more pigment (108 rhodopsin or molecules per rod) than do cones. Rods are so sensitive that a single photon can trigger a rod response. Rods are therefore well suited for night vision. Rhodopsin or visual purple has two absorption maxims: 350 and 500 nm. The spectral extinction curve for rods corresponds to that of rhodopsin, suggesting that rhodopsin is the chemopigment in rods. Rhodopsin consists of a glycoprotein (opsin) and a chromophore group (11-cis-retinal). Retinal is the aldehyde of vitamin A1 (retinol). The fovea only contains cones. Cones function in the daytime with maximal visual acuity and colour vision. The human eye possesses three types of cones, each with a specific pigment related to the three basic colours: red (erythrolab), green (chlorolab) and blue (cyanolab). The cones in the fovea do not contain cyanolab. When the human eye is fully adapted to darkness, its rods have open Na+-channels, and the resulting influx of Na+ maintains depolarised rods with a resting membrane potential of -40 mV. The rod cell synapses with bipolar and horizontal cells, and releases glutamate as long as the dark depolarisation is maintained. Na+ is continuously removed from the rod by the Na+-K+ pump. Inside the rod a special amplification takes place. Light absorption by a single rhodopsin molecule activates thousands of G-protein molecules (transducin), which then activate large quantities of cGMP phosphodiesterase in the discs. Each of these enzyme molecules catalyses the hydrolysis of cGMP to 5’-GMP at a rate of thousands per second. The reduction in [cGMP] closes the Na+-channels, and hyperpolarises the cell. The amplification mechanism is probably why the eye is capable of detecting a single photon. A similar cascade of reactions takes place in cones, when they are stimulated. Cones are so small that the hyperpolarization occurs rapidly. Each ganglion cell has a receptive field in the retina that is comprised of a number of photoreceptors. The fraction of a receptive field belonging to each photoreceptor is added to neighbour areas in order to obtain the receptive area of a bipolar or a horizontal cell. An on-bipolar cell is depolarised by white light, whereas an off-bipolar cell is hyperpolarised. Signals are transmitted from the photoreceptors to the ganglion cells as a graded response. These small receptive areas are summated to form a circular receptive field for each ganglion cell (Fig. 5-2). Ganglion cells can generate action potentials and transmit signals to the brain.
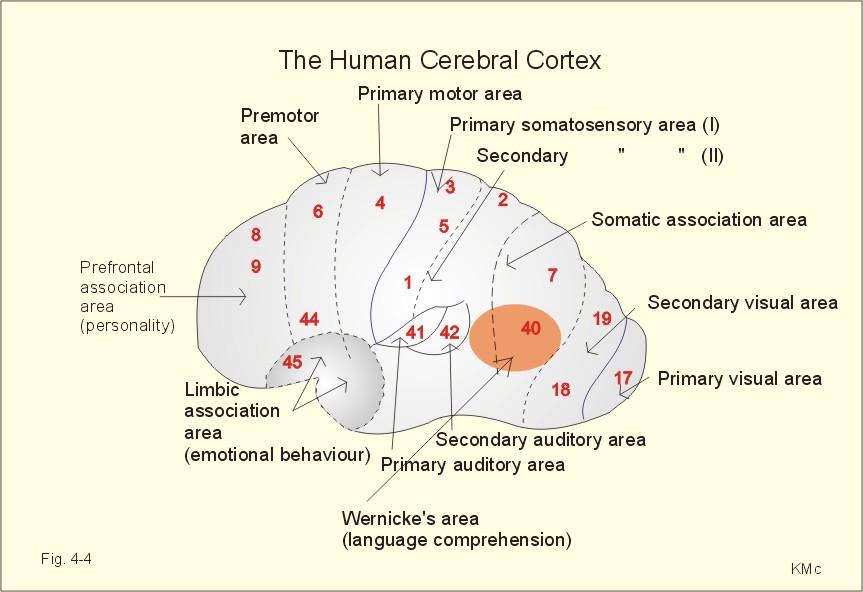
Fig. 5-2: Ganglion cell receptor fields in the retina. The ganglion cells can also produce transient or sustained reactions. These reactions are due to adaptation to light (decreased sensitivity with exposure) and lack of adaptation, respectively (Fig. 5-2). Ganglion cells in the fovea are connected to few or only one cone. Some ganglion cells are excited by blue light and inhibited by its opponent colour yellow. Other cells are excited by green and inhibited by the opponent colour red. This mechanism is the so-called colour contrast analysis of the retinal ganglion cells. Colour opponent neurons are found not only in the ganglion cells but also in the lateral geniculate nuclei. Retinal signals pass through the main visual pathway: the optic nerve, the lateral geniculate nucleus, the optic radiations (the geniculostriate tracts), the primary visual cortex, the pretectal area, the Edinger-Westphal nucleus, the oculomotor nerve and the ciliary muscle. Each point of the retina has a corresponding location in the dorsal lateral geniculate nucleus and in the visual, striate cortex (area 17). The nerve fibres in the optic nerve run so the upper quadrants of the retina are represented in the upper half of the nerve, and the lower quadrants in the lower half. Such a retinotopic map is present in the lateral geniculate nucleus and maintained throughout the visual pathways and in the visual cortex. The receptive field in the retina is maintained all the way to the cortex. This is the basis of fusion. The consequence is that the right striate cortex receives information about objects located in the left side of the visual field, and the striate cortex in the left hemisphere receives information about the right side of the field of vision. In general, each hemisphere of the brain is connected to sensory and motor activity of the opposite side. The lateral geniculate nucleus has three different pairs of neuronal layers (1-2, 3-4, 5-6). Ganglion cells from the ipsilateral (same side) eye projects to layers 2, 4 and 6, whereas ganglion cells from the contralateral eye projects to layers 1, 3, 5. The lateral geniculate nucleus is involved in integration and registration of pictures formed in corresponding areas of the retinal surfaces. Some neurons react to white light (with circular receptor fields), while other neurons react to opponent colours. When we jump from one highlight to another in the visual field, each jump is called a saccade. Selection of visual stimuli may be located in the lateral geniculate neurons (possibly performing gate control). Most of the neurons in the geniculate nucleus projects to the striate cortex by way of the optic radiations (geniculostriate tract). Neurons in a certain column of the lateral geniculate nucleus project to precisely the same part of the striate cortex (area 17). The lateral geniculate nucleus also receives information from the cortex (in particular the visual cortex) that is essential for selection of signals of particular interest. The striate cortex (area striata, area 17) is located around the calcarine fissure on the medial side of each occipital lobe. The optic radiation ends mainly in synaptic contact with simple cells in layer 4 of the striate cortex. Simple cells have on- and off-fields. Complex cells receive inputs from several simple cells, and hypercomplex cells receive inputs from several complex cells. Axons from one eye terminate in millions of functional units called ocular dominance columns consisting of about 103 neurons. Cortical neurons are arranged in orientation columns showing orientation selectivity for lines edges or bars. Other cortical neurons are arranged in direction columns showing direction selectivity. Colour blobs are interspersed among the other columns (see later). A large area at the occipital pole represents the macula, and the upper and lower half of the visual field is represented below and above the calcarine fissure. The upper layers of the superior colliculus perform visual processing. The deep layers produce eye movements. The cortical area V4 contains colour-sensitive neurons, and the visual association areas 18 & 19 (Fig. 4-4) contain many cells with complex functions. The absolute sensitivity depends upon the adaptive condition of the retina, the pupillary diameter, and the source of light (spectral composition, exposure time, and light source dimensions). The threshold for the completely dark-adapted eye is (7× 10-11) Watts/m2. Light adaptation is a decrease in visual sensitivity during constant stimulation. This occurs rapidly because the rhodopsin bleaches readily. Hence, in daylight (photopic cone vision) we are dependent on cones for vision. Night vision (scotopic rod vision) is extremely sensitive to light, because of dark adaptation. It takes at least 20 min in dark surroundings before the rods become fully adapted. In a dark movie theatre, we have scotopic vision with low visual acuity and colour blindness. As soon as the film is projected we experience partial light adaptation, so that the photopic cone vision is resumed. The trichromacy theory postulates that an appropriate mixture of the three basic colours can produce any colour: red, green and blue. The three types of cone pigments have different opsins, and opsins that differ from that in rhodopsin. Groups of cortical neurons called cortical colour blobs respond specifically to colour signals, and also receive signals from adjacent columns of the visual cortex. Cortical colour blobs are probably the primary stations for perception of colour, and they are found both in the primary and the secondary visual cortex areas. Perception of spectral opponent colour pairs is located in discrete colour blobs of the visual cortex. The three cone pigments are Erythrolab for red (maximal sensitivity at 555 nm), chlorolab for green (525 nm), and cyanolab for blue (450 nm). The absorption spectra of the photopigments overlap considerably. The three cone types are uniformly distributed in the retina, except in the fovea. Fovea has no cyanolab cones and no rods. This gives the fovea partial physiologic scotoma (ie, no blue vision and no scotopic dark vision). The real physiologic scotoma is the dark spot corresponding to the optic papilla. Inhibition of neighbour ganglion cells from on centre field ganglion cells is called lateral inhibition; it occurs also in the lateral geniculate nucleus or in the visual cortex. Lateral inhibition provides simultaneous contrasts and enhancement. Each colour-contrast neuron is excited by one colour and inhibited by the opponent colour. Opponent colours are red-green, yellow-blue, and green-purple. Contrast analysis begins already in the retina and is elaborated centrally in the lateral geniculate nucleus, the thalamus and the visual cortex. If there is a multilevel neural system for the analysis of colour mixing, we also need to assume the existence of a neural system for colour brightness, depending upon the intensity of the light. Healthy people are trichromats, because they have all three cone pigments. Spatial resolution or minimum separabile is the capacity of the eye to see two stimulated retinal areas as separated. In healthy young humans the spatial resolution is about 1/60 degree, depending upon luminosity, exposure time, patterns and opponent colours in the visual scenario. The most important factor limiting this capacity is the cerebral integration. Temporal, visual resolution is the capacity of the eye to see consecutive light stimuli as separate. Intensity is directly related to duration of perception of light. Contrast further decreases temporal resolution, a flash of light in the dark is perceived for longer than in bright surroundings. Temporal resolution is also determined by the wavelength of light. The eye is maximally sensitive at the absorption maxims of the three cone pigments and rhodopsin. The positive after-picture is a visual impression lasting longer than the stimulus. It is visible on a dark background following exposure of the eye to intense light. The negative after-picture follows the positive afterpicture as a dark shadow or as the opponent colour. The negative after-picture is due to adaptation of the area in the retina related to the picture. A flickering source of light liberates successive flashes so rapidly that they fuse, and appear to be continuous. In the darkness of a movie theatre we do not sense the flickering frequency of 24-48 frames each s, or those of a television screen with 50-60 frames per s. With increasing intensity of illumination the critical fusion frequency increases abruptly. This is why young persons can look directly into a neon light and see its flickering character even with 60-100 flashes each s. Accordingly, the cones of the healthy human eye have a critical fusion frequency around 60-100 flashes per s with optimal illumination. The photopic cones are much more sensitive to rapid alterations of light intensity than the rods. Movements in the visual scenery are depicted as opposite movements on the retina. Convergent inputs from the eyes result in depth perception (ie, stereopsis or stereoscopic vision). Stereopsis depends upon the medial, longitudinal fasciculus and the corpus callosum. These structures co-ordinate the movements of the two eyes. The two eyes are 7-8 cm apart, which causes slight disparities between their retinal images. Disparate receptive fields and thus excitation of specific cells in the secondary visual cortex probably exhibit the perception of depth. Distance evaluation requires high visual acuity and experience with objects of known size. Essential for the development of the baby’s brain is human milk proteins and long chain fatty acids in the mother milk. Protein deficiency from birth reduces formation of brain neurons and thus limits brain development including the development of visual capacity. Many vitamins and key proteins have hormonal and transmitter function in the brain, and lack of such substances in the critical growth period just after birth, results in irreversible damage. The action of endogenous nerve growth factor is necessary for the normal functional and anatomical development of the visual system. In the critical period of visual development, which is the first two years of life, the child must be exposed to a multitude of visual stimuli. This is necessary for the development of neurons and key substances that can record future visual stimuli. The ability to fuse the two optic fields is a process that has to be practised. This fact is an important basis for the treatment of cross-eyedness (strabismus). Cross-eyedness or squint (strabismus) is an eye disease, where the visual axes of the two eyes do not converge on the fixation point of the object simultaneously. Thus the retinal images do not fuse on corresponding areas on the two retinas. Since the fixation line only foveate in one eye, the patient can learn to suppress the other picture in the brain. Hereby, double vision is avoided at the expense of visual acuity. 2. The Auditory And The Vestibular System The two systems share the labyrinth, and transmit signals to the brain through the 8th cranial nerve. The two systems record fluid movements and use the so-called hair cells as mechanical transducers. Sounds are sense impressions that consist of complex mixtures of compression and decompression waves that can be broken down to pure tones by Fourier analysis. Pure tones are sinusoidal waves of a specific frequency (cycles per s or Herz = Hz) and amplitude. Sinusoidal waves can change phases. The normal human ear is sensitive to pure tones with frequencies between 10 and 30 000 Hz, in a young person. As people age, their capacity to hear high tones declines. This condition is termed presbyacusis. Sound propagates at 343 m/s in air at 20oC, although each single air molecule only moves a few mm in the direction of propagation. The unit of sound pressure (p) is Pascal (Pa). According to international convention the sound pressure level (SPL) is expressed in decibel (dB) - see Eq. 5-2. Any rise in the SPL of 10 dB implies a rise in sound pressure by a factor of 3, since the log of 3 is 0.5: 10 dB = 20 log 3 (Eq. 5-2). Speech has an intensity of 60-65 dB, and sounds that exceed 100 dB can damage the ear. A constant sound stimulation only results in minor adaptation. The human ear has the largest sensitivity around 1000-4000 Hz, the range for normal speech. The sound pressure waves in air are converted into sound pressure waves in the fluid column within the cochlea. The pressure wave in the air is transmitted via the tympanic membrane and the ossicles (malleus, incus and stapes), to the fluid of the cochlea. The foot plates of the stapes inserts in the oval window, and separates the middle ears from the fluid of the cochlea. The ratio of the effective surface area of the tympanic membrane to that of the oval window is 14:1, and the pressure is increased further by the differing lengths of the lever arms in the chain of ossicles. By this area-pressure amplification, hearing is improved by more than 25 dB. When the external ear is filled with water during diving, hearing is seriously reduced. Two muscles are found in the middle ear. They dampen movements of the ossicular chain when the ear is exposed to extremely high pitch sounds that can be anticipated. These muscles are the tensor tympani muscle supplied by the trigeminal nerve, and the stapedius muscle supplied by the facial nerve. Exposure to sounds above 90 dB elicits reflex contractions. The cochlea is composed of three tube systems coiled together to form a pyramid: scala vestibuli, scala media and scala tympani (Fig. 5-3). The part of cochlea beneath the oval window is called scala vestibuli, and it is filled with a fluid column termed perilymph.
Fig. 5-3: A cross section through one of the turns of the cochlea. The perilymph conducts the pressure wave to the basilar membrane, which is displaced within the endolymph together with the whole organ of Corti, which contains the hair cells. Each hair cell has 40-100 hairs (stereocilia). The hairs have different heights, and when the pressure wave displaces the hairs towards the tallest hair, the hair cells are depolarised. When the basilar membrane moves upward towards the scala media, the reticular lamina shifts upward and inward (Fig. 5-3), causing the hair cells to depolarise. Downward movement of the basilar membrane towards the scala tympani moves the reticular lamina downward and outward (Fig. 5-3). This movement hyperpolarises the hair cell membrane. The endolymph in the scala media has a potential difference of +80 mV with the perilymph as reference. The inside of the hair cell is -60 mV compared to the perilymph; this is a resting membrane potential about the same size as in most neurons. Thus the total potential difference between the inside of the hair cell and the endolymph in the scala media is -140 mV. This resting membrane potential is maintained by Na+-K+-pumps in the Stria vascularis (Fig. 5-3). Bending of the hair change the conductance of K+-ions through the apical hairy membrane, and this is how the resting membrane potential is changed. A current flow is produced through the hair cell from apex to base, which is resting on the basilar membrane (Fig. 5-3). This current flow or receptor potential can be recorded extracellularly with microelectrodes as the cochlear microphone potential (ie, the sum of receptor potentials from many hair cells). This potential has the same frequency as the acoustic stimulus, and the potential is analogous to the output voltage of a microphone. The cochlear microphone potential follows the sound stimulus without latency, without measurable threshold, and without fatigue in contrast to neuronal action potentials. Stimulated the hair cells release neurotransmitters (glutamate, aspartate) that excite the cochlear nerve fibres. Thus, the propagating action potentials are generated in the cochlear nerve fibres. A high frequency tone produces travelling waves along the basilar membrane. High tones travel only a short distance from the stapes along the basilar membrane to their resonant point, where the displacement amplitude of the basilar membrane is maximal (Fig. 5-4). Low frequency tones travel all the way to the apex of the cochlea (Fig. 5-4). The higher the tone frequency, the more basal located in the cochlea is the resonant point and its potential.
Fig. 5-4: Displacement of the basilar membrane illustrates the travelling wave theory (von Bekesy). The existence of such a maximum of the travelling wave is termed frequency dispersion. Since different frequencies excite differently located hair cells the argument is called the place analysis theory. The brain also utilises the temporal structure of the sound stimulus. This is the so-called periodicity analysis. The receptor potentials generate action potentials in the cochlear nerve (8th cranial nerve) that travel to the cochlear nuclei. Secondary neurons transfer the signals from here to the superior olivary nuclei that co-ordinates the two ears, or directly to the inferior colliculus through the lateral lemniscus (representing both ears). Axons from the inferior colliculus ascend to the medial geniculate nucleus of the thalamus. Axons from this thalamic nucleus form the auditory radiation, which terminates in the auditory cortex in the superior temporal gyrus (areas 41 and 42 in Fig. 4-4). High frequencies are projected to the rostral auditory cortex, and low tones to the caudal section. The duration of a sound stimulus is encoded in the duration of the neural signal, and its intensity by the level of neural activity. Projections from the auditory cortex also descend to the medial geniculate nucleus and the inferior colliculus. The oligocochlear bundle controls several sound impressions. Efferent stimulation through these pathways inhibits the sensitivity of these nuclei for sounds, while increasing their tone selectivity. This phenomenon, and a high degree of motivation, explains how a mother can hear her baby cry in spite of noise, and also how we can hear an individual in a crowd (the cocktail party effect). Localisation of a sound source depends upon the difference in time between the arrival of a low frequency sound signal to the left and right ears (time delay). The sources of low frequency sounds (below 2000 Hz) are localised by this time delay. The source of high frequency sounds is localised by the difference in sound amplitude arriving at each ear caused by the dampening of the sound intensity. Sounds in the region of 2000 Hz cannot be detected by either mechanism. On average, the distance between the two organ’s of Corti is about 0.16 m. Then, a sinusoidal wave or pure tone with exactly the same wavelength coming from one side of the head, is in phase when they reach the ears. This wavelength corresponds to the frequency of 2144 Hz (343 m/s divided by 0.16 m). In this instance the subject will be unable to determine the source of the sound. The vestibular system detects if the body is in balance. The sensory unit of the auditory-vestibular system is the membranous labyrinth, located in the petrous portion of the bony labyrinth. The membranous labyrinth contains endolymph and is surrounded by perilymph; it is composed of the auditory cochlear duct or scala media, and the balance regulating the Vestibular system. The vestibular system consists of three semicircular ducts and two otolith chambers (the utricle and the saccule). Each semicircular duct has a swelling termed an ampulla (Fig. 5-5).
Fig. 5-5: The spatial orientation of the three semicircular ducts in the upright person (left). The horizontal duct is not drawn. The membranous labyrinth is shown to the right. The semicircular ducts consist of a horizontal duct, a superior and a posterior duct at right angles to each other, so that they cover all three planes in space. The semicircular ducts all communicate with the utricle. The utricle joins the saccule, which receives new endolymph from the cochlear duct. The sensory organ of each utricle and saccule is called a macula. The sensory organ of each semicircular ampulla is the crista ampularis. Each macula contains thousands of hair cells. Vestibular hair cells each have many stereocilia (hairs) on their apical surface just as cochlear hair cells do; however, they also have a large stereocilium called kinocilium. The hairs are imbedded in a gelatinous substance, the otolithic membrane that also contains earstones or otoliths. These otoliths increase the specific gravity of the otolithic membrane to twice that of the endolymph. Thus their hair cells are sensitive to linear acceleration such as gravity and to static equilibrium control, but not to angular accelerations of the head. The macula of the utricle is located in the horizontal plane, and the macula of the saccule in the vertical plane. Each crista ampularis consists of many hair cells. Here the hairs are imbedded in a large gelatinous substance termed a cupula. The cupula occludes the lumen of the ampulla completely, and its material has the same specific gravity as the endolymph. The cupula is concerned with equilibrium control during motion and with angular acceleration (rotation of the head), but is unaffected by linear acceleration. When the stereocilia are bent toward the kinocilium, the conductance of the apical cell membrane increases for positive ions, and the hair cell becomes depolarised. Bending the stereocilia in the opposite direction hyperpolarizes the cell. The depolarised hair cell releases glutamate or aspartate and increases the discharge rate of the nerve fibre with which it synapses. The utricles and saccules are sensitive to linear accelerations. When we suddenly thrust our body forward, the otolithic membranes fall backwards on the cilia of the hair cells until the thrust stops. Then, the otolithic membranes fall forwards. The signals to the brain make us feel as if we were falling backwards. Therefore, we lean forward until the otolithic membranes are in balance. This paragraph deals with 1. Refractive disorders, 2. Colour blindness, 3. Visual field defects, 4. Mental blindness, 5. Deafness (hypacusis), 6. Nystagmus, and 7. Kinetosis. (myopia, hypermetropia, astigmatism, presbyopia, and cataract). Near-sighted (myopic) patients usually have elongated eyeballs. More rarely, myopia can be caused by too high refractive power in the lens system. Myopic persons can only foveate diverging light waves - both from F and N (Fig. 5-1). The images of distant objects are focused in front of the retina, and the image is blurred on the retina. Both F and N are located in front of the eye. Concave lenses (-D) accomplish correction. The weakest concave lens compatible with optimal visual acuity is the best correction, as the accommodation is eliminated. Hypermetropic or far-sighted persons usually have shortened eyeballs, and F is always behind the eye. In rare cases hypermetropia can also be caused by insufficient refractive power in the un-accomodated eye. The absolute hypermetropic eye can only focus images of distant objects behind the retina (Fig. 5-1). The facultative hypermetropic eye can focus converging light beams on the retina without accommodation (rest in Fig. 5-1). This patient can read the Snellen letters without problems; they also foveate diverging light beams by accommodation, but then the patient gets eyestrain due to fatigued ciliary muscles. Convex lenses (+D) correct hypermetropia. The strongest convex lens compatible with optimal visual acuity is the best correction, as the accommodation is eliminated. Astigmatism is a refractive disorder of the eye, in which the curvatures of the cornea or lens are different along different meridians. The different meridians therefore have different focal distances. Therefore, astigmatism can be corrected with cylinder lenses that correct the curvature differences. Presbyopia is called old man’s sight. The far point remains where it is, so the un-accomodated refraction is unaltered. The ability to accommodate is changed, so that N approaches F. With age, the lenses of most people loses its elasticity, and hence their ability to assume spherical shape. The lens is the organ in our body with the highest protein concentration. Alterations of lens proteins probably cause progressively increasing stiffness of the lens. The accommodative power decreases from 14 D in a child to less than 2 D at the age of 50. The patient’s eye becomes incapable of accommodation for near vision and reading. Convex lenses correct presbyopia. Cataract is an eye disease, where the vision is blurred by an opaque lens. Precipitation of lens proteins can occur in several ways. It is often due to oxidative processes. The lens needs oxygen, but strong sun light or radiation can oxidise lens proteins in unprotected eyes. The oxidation is enhanced by hyperbaric oxygen therapy and by high blood [glucose] in diabetics. Oxidants in the food may be the cause in some patients. Antioxidants, such as vitamin A and D, seem to protect against the loss of transparency in long-term studies. Today, excellent surgical techniques are used to eliminate the opaque lens and re-establish normal refraction. The three colour genes are located on an X chromosome. Females have two X-chromosomes, and colour blindness is rare among females. Colour blindness is inherited from the father - via the daughter - to her son. The trait is recessive and sex linked. The total incidence is about 8% of the male and 0.5% of the female population. Monochromats lack all three or two cone pigments, an extremely rare disorder. Dichromats lack one of the three cone pigments. Proteus is the first or red component, so protanopic people are blind for the red part of the spectrum. They cannot separate red and yellow signals in traffic. Deuteranopic patients are blind for the second or green colour, and tritanopics are blind for blue - the third basic colour. Abnormal trichromats have a reduced amount of one cone pigment: Protanomalous trichromats lack erythrolab, deuteranomalous (the most frequent type) lack chlorolab, and tritanomalous lack cyanolab. Visual field defects are caused by interruptions of the visual pathways. Hemianopsia means loss of vision in half of the visual field of both eyes. The loss of vision refers to the visual field, and thus to the contralateral half of each retina (shown with two colours in Fig. 5-6). Homonymous hemianopsia means that the same side of the visual field for each eye is defective. Corresponding halves of each retina has lost vision (black in the illustration). Homonymous hemianopsia occurs from lesions of the entire optic tract, the lateral geniculate body, the optic radiation, or the entire visual cortex of the contralateral hemisphere (Fig. 5-6). A lesion of the striate cortex often spares the large macular area at the occipital pole. This results in a disorder termed homonymous hemianopsia with macular sparing (Fig. 5-6). Partial lesions may cause quadrant-anopsia. Heteronymous hemianopsia can be bitemporal or binasal (Fig. 5-6). Bitemporal hemianopsia results from damage of the optic nerve fibres as they cross the optic chiasm (Fig. 5-6). An expansively growing pituitary tumour, perhaps related to acromegaly, can damage crossing fibres, originating from ganglion cells in the nasal halves of each retina. Expansion of the tissues surrounding both carotid arteries is a rarity, which can damage nerve fibres from the temporal halves of each retina, and cause binasal hemianopsia (blind parts of the visual fields shown in Fig. 5-6 are marked with red - or with black)..
Fig. 5-6: Visual field defects. Lesions are shown with bars. As long as the patient sees with both eyes, he may not experience any visual defect caused by damage to non-corresponding areas of the retina. Localised blindness or scotoma is caused by a lesion of the retina in one eye, or by partial interruption of the optic nerve. Interruption of the entire optic nerve results in complete blindness or anopsia (Fig. 5-6). Ophtalmoscopy is an important diagnostic tool able to establish both eye disorders and systemic diseases.
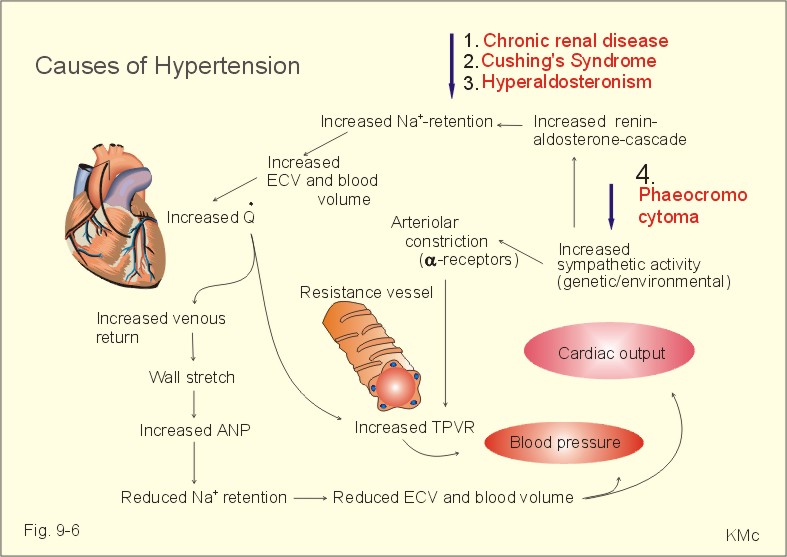
Fig. 5-7: The eye background (fundus) of the right eye in a healthy person. – A typical hypertensive eye background is shown in Fig. 9-6. The normal ophtalmoscopic picture of the fundus is seen in Fig. 5-7. The papilla is clearly visible with the central artery and vein, and the cone-filled fovea is located to the left. The papillo-macular nerve bundle connects to the cones of the macula, but this bundle is invisible. This person has a small pigmented area along the lateral side of the papilla (Fig. 5-7). Bilateral temporal lobe lesions can lead to the Klüver-Bucy syndrome. In this condition, the temporal cortex, hippocampus and the amygdaloid body are damaged. The Klüver-Bucy syndrome includes mental blindness (visual agnosia). Mental blindness is the inability to recognise objects seen. Besides mental blindness, the syndrome consists of loss of short-term memory, and hypersexual behaviour incompatible with normal social adaptation. This hypersexual behaviour is related to the visual agnosia. Damage to visual areas of the temporal cortex alone causes isolated visual agnosia. Visual agnosia or mental blindness, is lack of the ability to combine the seen object into a concept. This visual agnosia can be colour-agnosia (acromat-agnosia) or face-agnosia (prosop-agnosia). Nerve deafness is caused by impairment of the cochlea, the auditory nerve or the nucleus. Chloramphenicol, kinin and streptomycin can damage the cochlea. These drugs can cause hearing loss or deafness for all sound frequencies. Deafness to specific frequencies is caused by localised damage of the basilar membrane. This is typical for rock and beat musicians, soldiers, and airline pilots. The nerve deaf patient has a hearing loss when tested both by air conduction through the middle ear, and bone conduction through surrounding bone structures. A certain type of nerve deafness for high tones develops among older persons (presbyacusis). Conduction deafness is caused by impairment of the mechanical conduction of sound into the cochlea. A hereditary disease called otosclerosis is due to fixation of the faceplate of the stapes to the oval window. Otosclerosis, blockade of the external ear with ear wax, otitis media, damage of the tympanic membrane, and of the ossicles all cause conduction damage to hearing. Persons with conduction damage have normal bone conduction. Nystagmus is a disorder with abnormal involuntary movements of the eyeballs. Opto-kinetic nystagmus occurs when travelling in a train or a car. The eyes remain fixed on an object long enough in order to gain a clear image. The semicircular ducts cause the eyes to rotate in the direction opposite to the direction of travel. Optokinetic nystagmus involves the vestibular nuclei, the medial longitudinal fasciculus, and the oculomotor nuclei. Post-rotatory nystagmus is observed in a person sitting in a rotating chair. This is the physiologic adequate stimulus for nystagmus. Caloric nystagmus refers to the horizontal reflex movement of the eye when the external ear is flushed with hot or cold water. The fast phase of the nystagmus is directed away from the ear flushed with cold water, and towards the ear flushed with hot water. The caloric nystagmus test is preferable to the post-rotatory test for testing the nystagmus reflexes, because it examines one ear at a time, and is more convenient. 7. Kinetosis or transportation sickness Many types of transportation, which subjects passengers to rapid changes in the direction of motion, elicit kinetosis. Kinetosis is a disorder with vertigo, nausea and vomiting. The disorder is triggered from the vestibular system, provided that the cerebellar function (the flocculo-nodular lobe) is intact. The flocculo-nodular lobes are linked to the equilibrium control of the semicircular system. Persons with destroyed semicircular canals or with destroyed flocculo-nodular lobes can be completely protected from kinetosis at the expense of lost equilibrium during motion. The accommodative power of the eye is the rise in refractive power from un-accomodated to the maximally accommodated condition: Eq. 5-1: Accommodative power = 1/F - 1/N. F and N are the far- and the near point, respectively. A child of 10 years has the high accommodative power of 12-14 D, a 20-year-old person 10 D, and a 60-year-old person 1 D. According to international convention the sound pressure level (SPL) is expressed in decibel (dB): Eq. 5-2: Sound pressure level (dB) = 20 log p/po. The actual pressure is p, and the threshold for sound pressure is po . The threshold for sound pressure is 20 mPa in air (po) at 1000 Hz in a sound tight chamber for a healthy person. This pressure corresponds to a sound effect of 10-12 Watts/m2. I. The following five statements have True/False options: A. The fovea has no cyanolab cones and no rods. B. C. D.
II. The following five statements have True/False options:
A 30-year old female complains of eyestrain and frontal headache during reading - sometimes followed by nausea and vomiting. The patient is placed 6 m (20 feet) from the Snellen test chart. She is able to read line 6, which is the letter size read by a normotropic eye. Now thin convex lenses are placed in front of her eyes, but she can still read line 6. The diopter of the strongest convex lens with which she can still read line 6 is +4 D for both eyes. These converging light rays must be directed against the far-point (F). F must be located behind the eyes at a distance of ¼ m. Examination with concave lenses reveals the strongest concave lens by which she can read line 6 to be -3 D or N = -1/3 m (in front of each eye).
A patient with a hearing loss of 26 dB is working in a power station, where the daily sound intensity is 100 dB and the air temperature is 20oC. 1. Calculate the ratio between the sound pressure in the powerhouse, and the sound threshold pressure for a healthy person.
A 9-year-old girl suffers from facultative hypermetropia. She is placed 6 m from the Snellen test chart and asked to read line 6, which is the letter size read by a normotropic eye. When thin convex lenses are placed in front of her eyes, she can still read line 6. The diopter of the strongest convex lens with which she can still read line 6 is +5 D for both eyes. Examination with concave lenses reveals the strongest concave lens by which she can read line 6 to be -4 D.
A 40 year old male diabetic has an accommodative power of 10 D. His near point (N) is located 0.05 m in front of the eye (- 0.05 m).
Try to solve the problems before looking up the answers.
Berardi, N., A. Cellerino, L. Dominici, M. Fagiolini, T. Pizzorusso, A. Cattaneo, and L. Maffei. "Monoclonal antibodies to nerve growth factor affect the postnatal development of the visual system." Proc. Natl. Sci. , USA, 91 (2): 684-688, 1994. Stryer, L. "Cyclic GMP cascade of vision." Annual Rev. Neuroscience 9: 87, 1986. Brodal, A. "Neurological anatomy in relation to clinical medicine." Edition 3. New York, 1981, Oxford University Press. Von Bekesy, G. "Experiments in hearing." New York, 1960. Mc-Graw-Hill.
|
||







.jpg){kind=link}
{kind=link}
{kind=link}
Click here to introduce your comments or contributions